Role : User Experience Designer
Duration : 4 Weeks
Expertise : Secondary User Research • Service Design • Interaction Design
Project Type : Speculative Service Design Concept
Location : Bengaluru, India
It started with a siren I couldn’t get out of my head
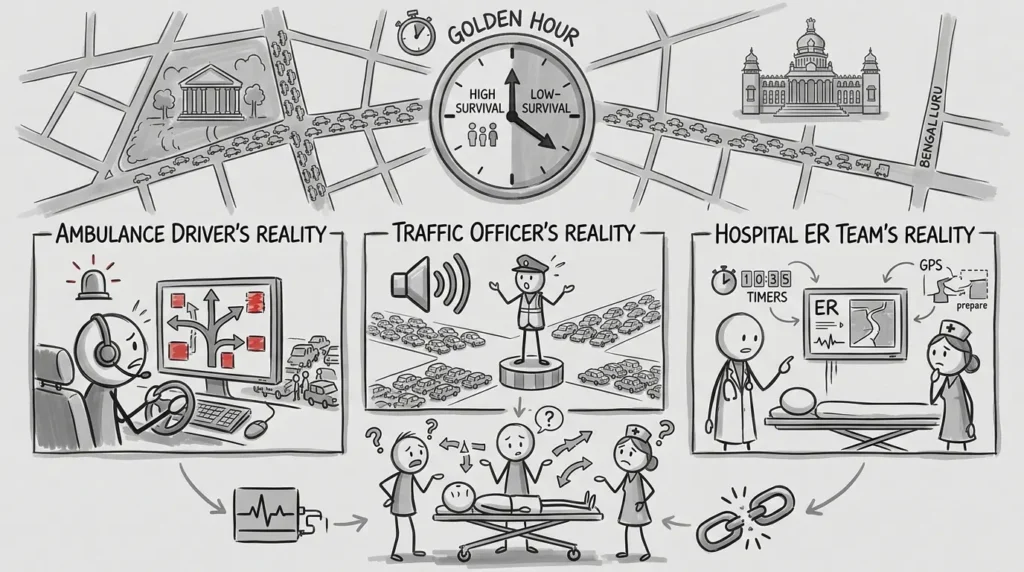
In emergency medicine, there’s a window called the Golden Hour. the first sixty minutes after a critical incident, where every extra minute stacks the odds against survival.
In Bengaluru, that hour runs straight into some of the worst traffic in the country. And the more I looked into it, the more I realized the ambulance itself wasn’t really the problem. It was that nobody in the chain like the driver, the traffic officer, the hospital was working off the same information. The driver didn’t know which roads would actually clear. The traffic officer found out an ambulance was coming when he heard the siren, which by then meant fifty cars were already in the way. And the ER was preparing off a GPS ETA that changed every few minutes, so ‘prepare for the patient’ mostly meant guessing.
Three people with three completely different realities doing everything they can trying to save the same life.
The question that reframed the whole project
I went in assuming this was a routing problem like better maps, smarter navigation. It wasn’t. Every stakeholder I mapped had visibility into their own slice of the journey and nothing else. So the real question became:
How might we give everyone in the emergency response chain the same real-time picture, so patients reach treatment faster?
That single shift from ‘help the ambulance move’ to ‘help everyone see the same thing’ is what LifeLane is built around.
Meeting the people who’d actually use this, aka the stakeholders
A note on how I got here: this was secondary research (desk research) and not live interviews. Kiran, Ramesh and Dr. Anjali are composites which were built from published accounts, ride-along reporting and interviews with ambulance drivers, traffic police and ER staff that I found in news coverage and public health writing on Bengaluru’s emergency response system. I gave them names because the quotes are real patterns and not because I sat across from three specific people.
I spent time understanding three very different jobs happening under very different pressure:
Kiran, an ambulance driver, wasn’t short on maps. He was short on certainty. ‘I don’t need another map. I need to know which road will actually move.’
Ramesh, a traffic officer, standing in harsh sun making split-second calls, told me plainly: ‘By the time I hear the siren, there are already 50 vehicles blocking the junction.’ He didn’t need a dashboard. He needed a warning.
Dr. Anjali, an ER coordinator, was stuck replanning every few minutes because the ETA kept shifting under her. She just wanted a number she could trust.
None of them wanted more information. They wanted the right information at the moment they could still act on it.
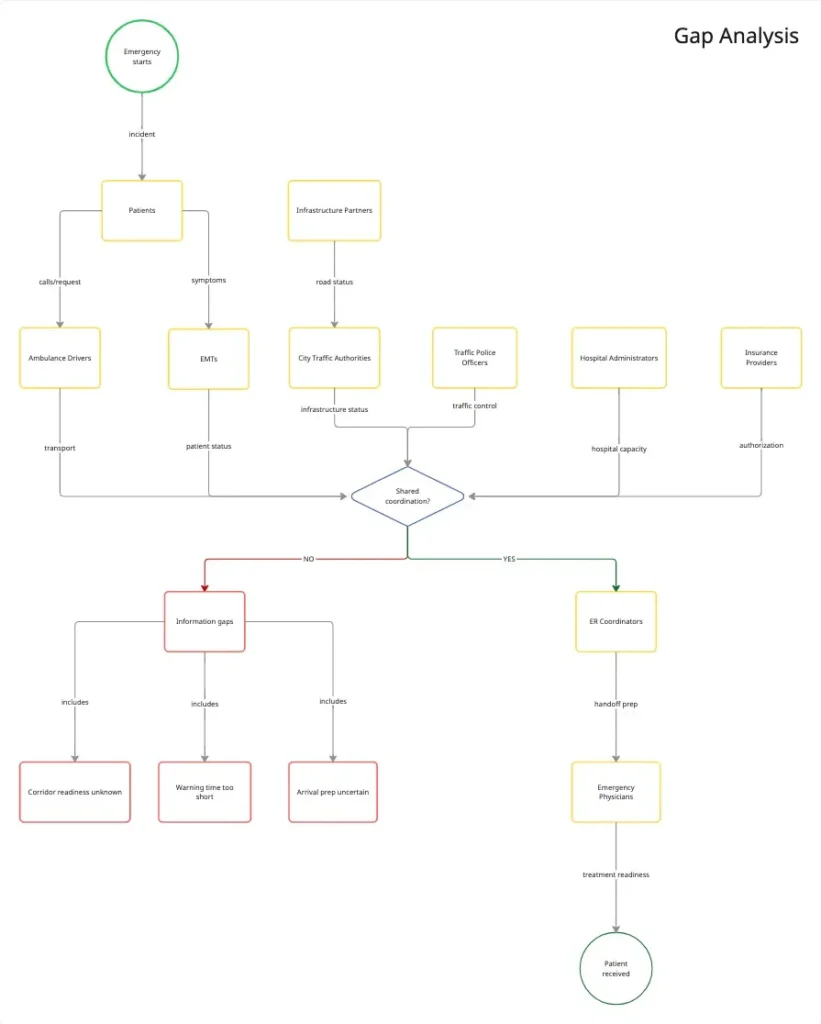
The challenge was not navigation. The challenge was coordination.
Each stakeholder operated with different information, different priorities and different visibility into the patient journey.
Information Gap: Nobody had a shared picture of where the ambulance actually was. The ambulance couldn’t predict which corridor would be ready for it.
Timing Gap: Traffic officers found out too late to do anything but react. By the time they had warning, the moment to act had already passed.
Reliability Gap: The ETA moved so often hospitals stopped trusting it, which meant they couldn’t actually prepare for the patient.
Building a Better-Coordinated Emergency Response System
Research revealed a critical service gap: No stakeholder had a shared source of truth regarding ambulance movement.
This led to the core opportunity: Create a city-wide coordination layer between ambulances, traffic officers, and hospitals.
Three opportunities emerged:
Earlier Traffic Awareness: Provide traffic officers with actionable notice before ambulance arrival.
Reliable Location Confidence: Reliable Location Confidence: Give everyone in the chain a number they can actually trust and not one that shifts every few minutes.
Better Hospital Readiness: Enable hospitals to prepare resources based on reliable arrival predictions.
What LifeLane is designed to do
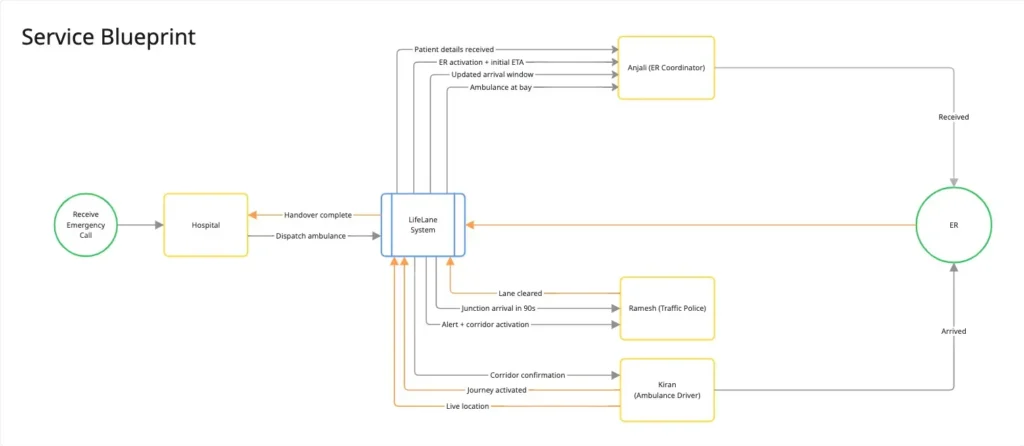
This is the concept end-to-end of how LifeLane connects hospitals, ambulances and traffic control into one shared corridor of information from dispatch to handover, if it were built.
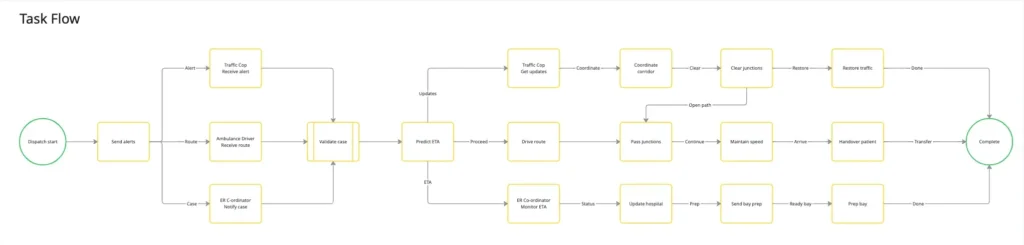
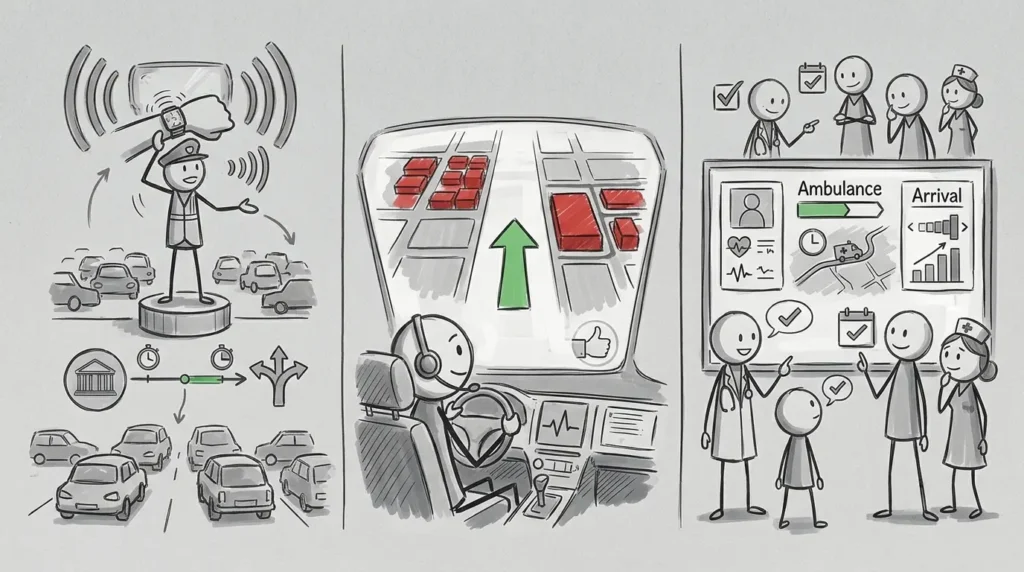
- Dispatch the hospital activates a LifeLane corridor, and every stakeholder is instantly looped into the same journey.
- Transit the system tracks the ambulance and predicts, junction by junction on when it’ll arrive.
- Corridor creation traffic officers get a heads-up like ‘Ambulance approaching from MG Road, arrival in 90 seconds’, time to actually clear a path instead of reacting to a siren.
- Hospital prep the ER gets a reliable arrival window instead of a flickering ETA, so the team is ready before the doors open.
- Arrival handover happens with far less scrambling on either end.
Designing for people who don’t have time to look down
The hardest constraint wasn’t the technology, it was that none of these users could afford to stare at a screen.
For traffic officers, I stripped everything back to what a person can absorb in under a second while directing live traffic: haptic alerts, voice guidance, and landmark cues instead of a map. Not ‘here’s a route’ more like just ‘Passed Richmond Circle. Approaching Trinity Junction. 90 seconds.’
For ambulance drivers, more information wasn’t the goal, confidence was. The system surfaces cleared routes and reroutes around congestion automatically so decisions get simpler, not busier.
For hospitals, it came down to trust. A live command view shows patient status, transport progress and an arrival window the team can actually plan around.
Where this could break
Because LifeLane never left the design stage, I couldn’t test it against real traffic or real hospitals so instead I tried to break it on paper. A few places worried me: Traffic officers are already juggling five things at once. If LifeLane’s alert arrives at the same moment as three other decisions, it doesn’t get ignored, it adds to the exact overload I was trying to remove. The fix isn’t a louder alert, it’s making sure the system knows when not to interrupt.
The whole corridor depends on GPS and network coverage staying reliable in dense traffic, which in Bengaluru is optimistic at best. If the signal drops mid-corridor, an officer who cleared a path based on a prediction that never arrives loses trust in the system fast and trust for once lost, doesn’t come back with a software update.
And coordination systems live or die on adoption being close to universal. If even one hospital or one traffic zone opts out, the ‘shared picture’ everyone else is relying on has a hole in it exactly where they need it most.
What this project actually is
I want to be upfront about what LifeLane is and isn’t. This is a coordination layer, a way of rethinking how information should move between three groups who currently don’t share any or not a finished app with usage numbers to point to.
That was a deliberate choice. I was more interested in the systems question, what would it take for a traffic officer, an ambulance driver, and an ER coordinator to act on the same truth at the same moment, than in shipping a single interface? The output here is the logic connecting them, not a product you can download.
So there’s no adoption curve or time-saved metric to report and I’d rather say that plainly than dress up a hypothesis as a result. What I can show is the reasoning: where the coordination breaks down today, what each person actually needs to act in time and a structure that closes those gaps. If this moved into a pilot, the next step would be exactly the failure points above.

What I took away from this
The most important design work here wasn’t a single screen, it was rethinking how information moves across an entire healthcare ecosystem. Reframing this as a coordination problem, not a navigation problem is what unlocked the real opportunity: continuity of care across organizations that had never shared a system before.
If there’s one thing this project left me with, it’s this : in healthcare, the system coordinating behind the scenes often matters as much as the clinical expertise in front of the patient.